This video presents: Regulation of the Blood Flow. Long Term Flow is not covered in this chapter. Acute blood flow types i.e. Extrinsic and Intrinsic. Metabolic and myogenic theory of the intrinsic blood flow. Role of the blood vessels in the blood flow including ERDF and Endothelin.
CVS PHYSIOLOGY LECTURE # 9 STUDY NOTES:
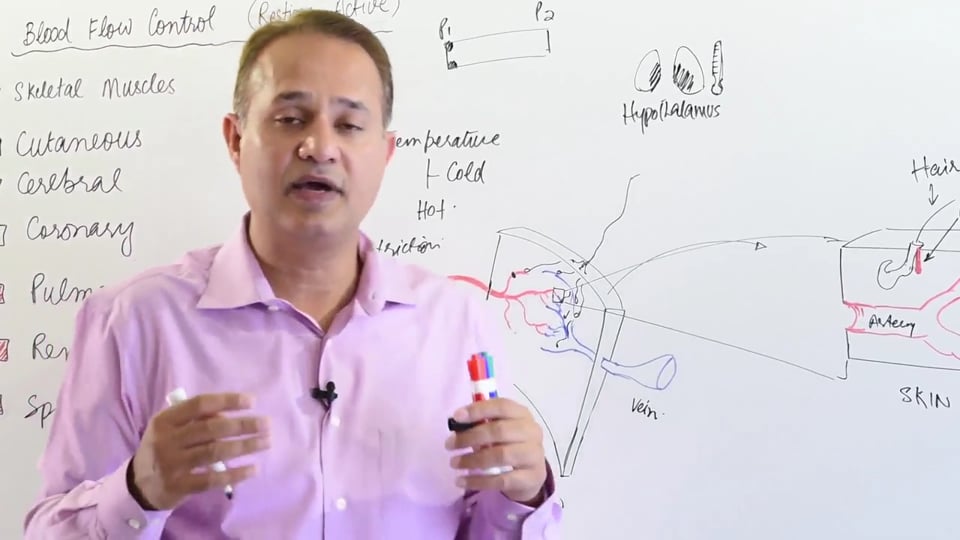
AUTOREGULATION OF BLOOD FLOW
When we talk about autoregulation, it's not the blood pressure we are talking about but it's rather the blood flow over a changing pressure which is being regulated. In terms of hemodynamics, the flow across a blood vessel is determined by the pressure gradient across its two ends, assuming that the vessel diameter (resistance) remains unchanged.
The equation for blood flow across a vessel is as following:
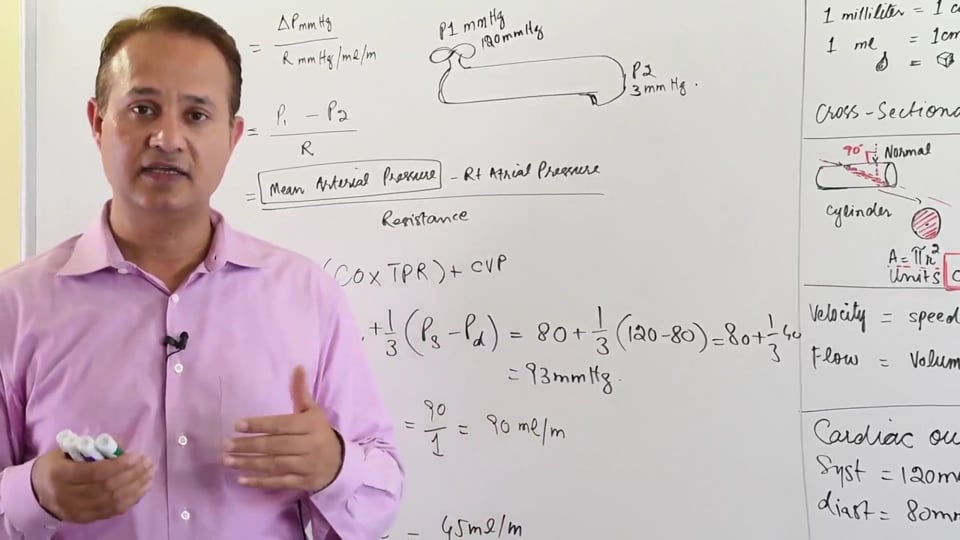
➢ Flow = ΔP/ R
Flow = [P1 - P2]/ R
Where,
ΔP = Pressure gradient
R = Resistance to blood flow across the vessel
Blood flow change can occur if any of the following factors change:
• Blood volume
• Vessel diameter i.e., the resistance to blood flow changes
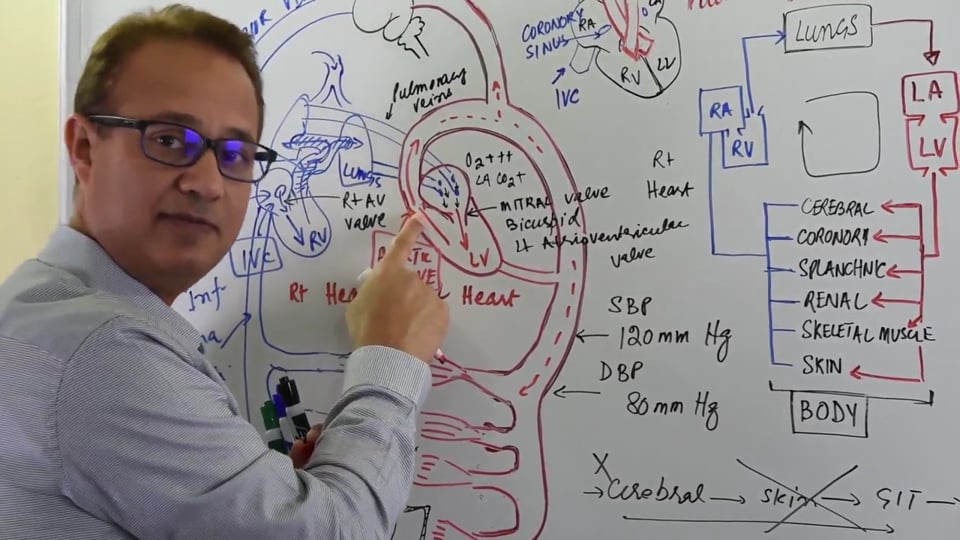
It's important to understand that any pressure changes of the blood result in flow changes across capillaries supplying blood to the tissues. If the flow changes, there can be derangements in the perfusion of the tissues. One of the major functions of cardiovascular system is to provide optimal perfusion to the tissues. Perfusion ensures optimal delivery of nutrients and oxygen and removal of metabolic waste products from the tissues. So for this reason, if there are any pressure changes then the body will try to regulate the blood flow accordingly in order to maintain optimal perfusion of the systemic tissues. So it's safe to assume that it is the blood flow which is regulated as part of hemodynamics, not the vascular resistance (arteriolar diameter). In fact, vascular resistance is altered in order to regulate blood flow.
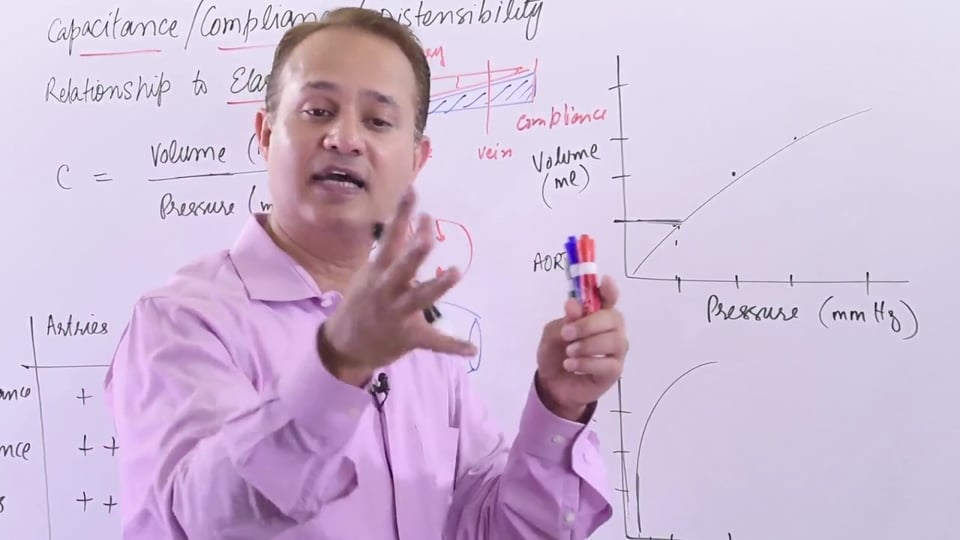
Autoregulating tissues are those which exhibit local blood flow regulation, thereby maintaining a constant blood flow even if the perfusion pressure changes (MAP). The blood pressure range over which an autoregulating tissue can maintain a constant blood flow is called the autoregulatory range. The autoregulatory range in our body is from a MAP of 70 mm of Hg to 175 mm of Hg. Outside the autoregulatory range (MAP < 70 and MAP > 175), the flow doesn't remain constant. There is a proportional decrease or increase in flow if the MAP falls below 70 mm Hg or increases above 175 mm Hg, respectively.
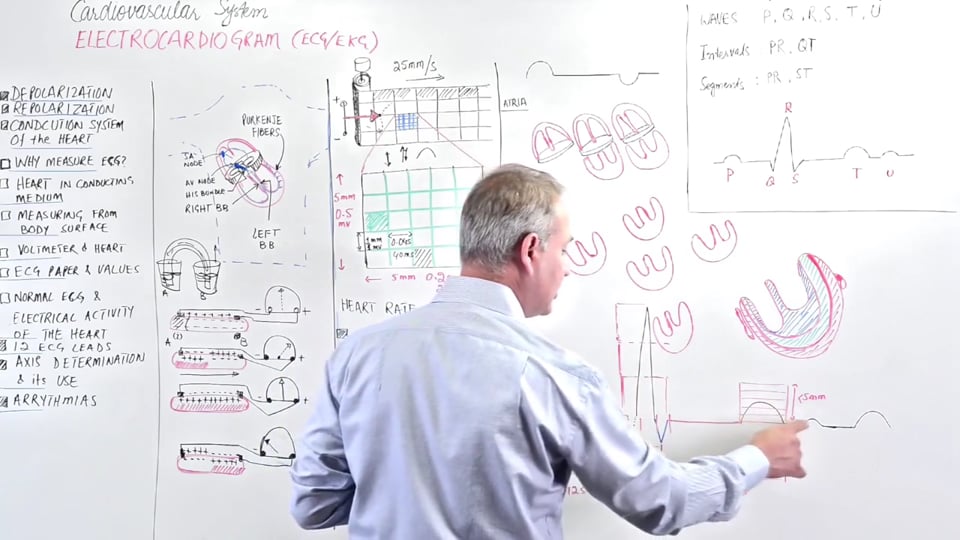
Following is a brief summary of what's happening to the flow at points A, B & C on the autoregulation graph in drawn in the lecture:
• Point A: This point falls outside the lower limit of autoregulatory range (MAP < 70). Up till point A, as the MAP increases from 0 to 70 mm Hg, the blood vessel is maximally dilated. The blood vessel is as relaxed as possible and as the blood flow through it increases, there's a proportional increase in the blood pressure of the vessel.
• Point B: This point falls within the autoregulatory range. The increased blood pressure resulting from an increased flow results in smooth muscle contraction of the vessel. This reduces the diameter of the blood vessel and the flow is kept constant. The blood vessel continues to constrict until the upper limit of the autoregulatory range is reached
(MAP = 175).
• Point C: This point falls outside the upper limit of autoregulatory range (MAP > 175). Outside this range, the vasculature can't constrict any further so the blood flow can't be kept constant anymore. Hence, any further increase in the blood pressure will always be accompanied by an increase in blood flow.
NOTE: The blood flow is primarily governed by dilating or constricting the smooth muscle within the walls of the arterioles, provided that other factors such as viscosity of blood, blood volume and other physiological factors are kept constant.
There are several types of blood flow regulations:
1) Long term regulation: This is done by achieved by increasing the size and diameter plus increasing the number of blood vessels. It can take from months to years to achieve such kind of a change. This long term blood flow regulation will later be discussed in a separate lecture.
2) Acute regulation: This responds to the local needs of a metabolically active tissue. Only those tissues which require greater blood flow owing to their metabolic activity receive a greater blood flow. This ensures that the blood flow to whole of the body is not increased if a particular tissue needs more perfusion. Overall, this makes sure that the workload on the heart doesn't increase too much. Acute regulation of blood flow is further divided into the following types:
• Extrinsic regulation involves SANS and PANS input to regulate vascular diameter. Extrinsic regulation will be discussed later in a separate lecture.
• Intrinsic regulation involves mediators released from the tissue itself which ensure that adequate perfusion to the tissue is maintained. Autoregulating tissues fall under this category of tissues which have their perfusion regulated by the tissue itself, and examples of these are as following:
▪ Cerebral circulation
▪ Coronary circulation
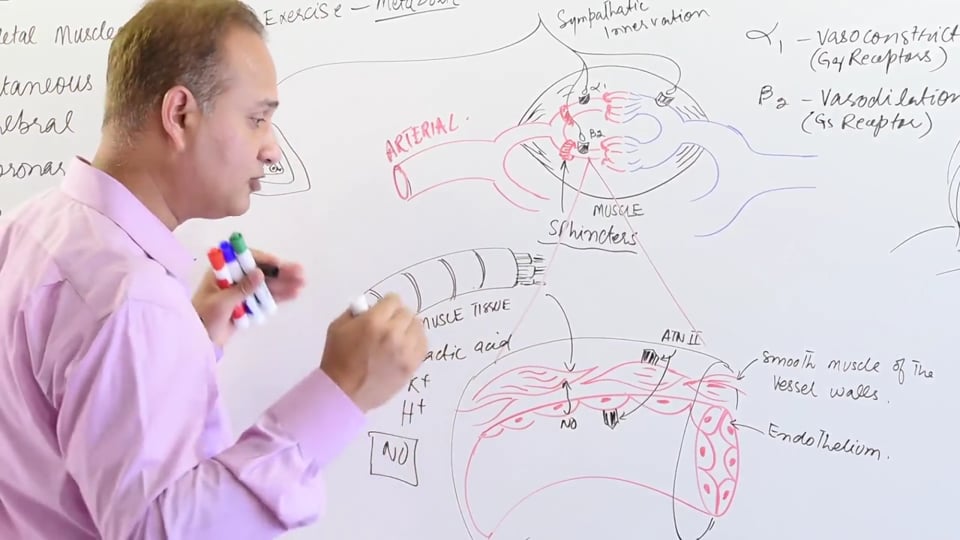
▪ Skeletal muscle vasculature (during exercise)
▪ Renal Circulation
There are two major mechanisms which are used toexplain intrinsic regulation (autoregulation). These include the metabolic and myogenic mechanisms. Both these mechanisms cause vasodilation of the blood vessel which leads to an increase in the perfusion of the tissues supplied. Metabolic mechanism is the primary theory which regulates the local vascular diameter of the vessel. The myogenic theory is the subordinate theory to the metabolic theory.
3) Vascular system control on the blood flow: It is also involved in the regulation of blood flow to tissues. It falls both under both the intrinsic and the extrinsic categories, so it's discussed separately here. Certain substances suchas EDRF (endothelium derived relaxing factor) and Endothelin are released which act on the endothelium itself and subsequently regulate the blood flow to the tissues. EDRF acts to cause vasodilation whereas Endothelin causes vasoconstriction.
VASCULAR SMOOTH MUSCLE CONTRACTION OR RELAXATION AND THE RESULTANT CHANGE IN BLOOD FLOW
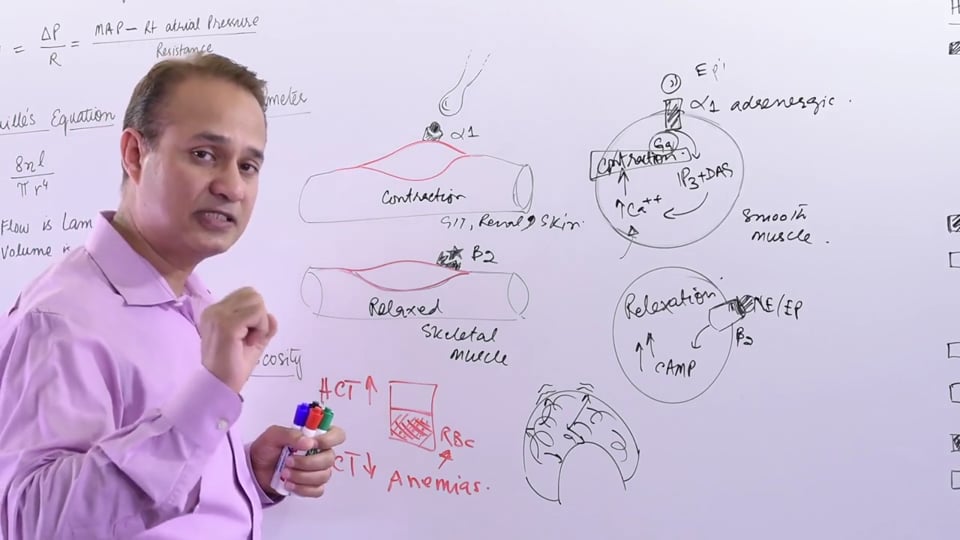
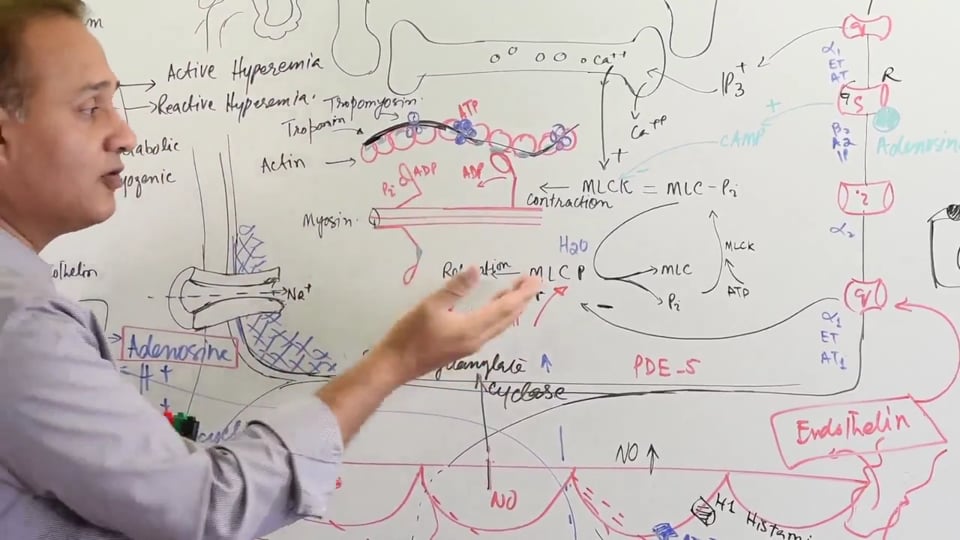
The blood supply to a tissue brings oxygen and nutrients and removes the carbon dioxide and other waste products away as part of the perfusion. The blood vessel is surrounded by smooth muscle within its wall. Relaxation of vascular smooth muscle causes vasodilation, allowing more blood flow through the blood vessel. On the other hand, the contraction ofvascular smooth muscle results in vasoconstriction of the blood vessel which decreases the diameter of the vessel and reduces forward flow. The cascade of events which occur during the vascular smooth muscle contraction are explained below:
1) On the smooth muscle surface membrane there are T-tubules along which the action potential travels.
2) Sarcoplasmic reticulum is the site for intracellular calcium, which is released when depolarization of the smooth muscle cell occurs.
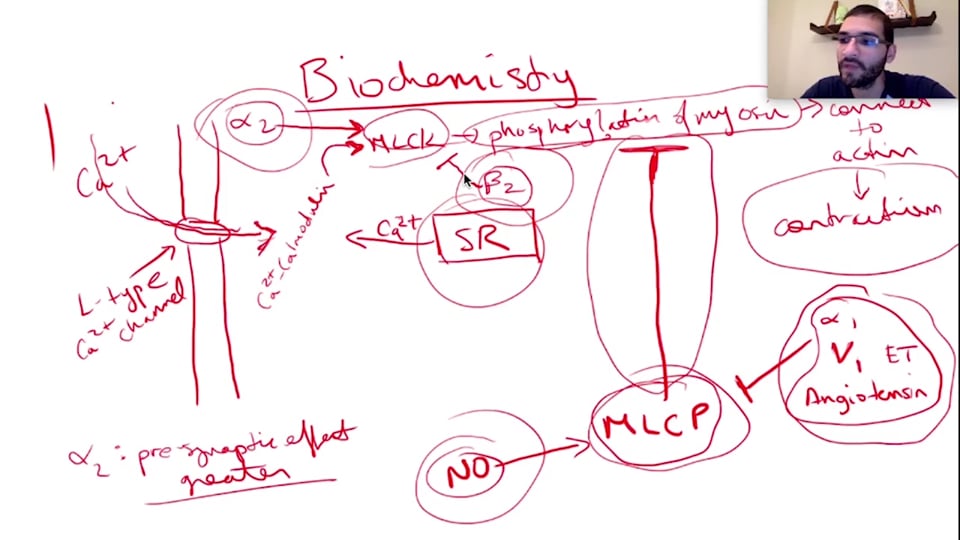
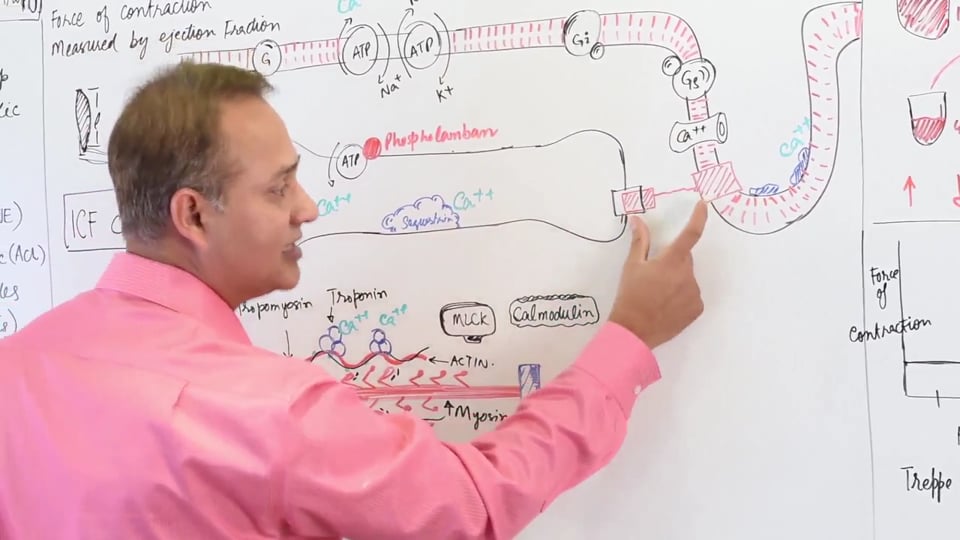
3) Calcium is released from the sarcoplasmic reticulum. This increases the intracellular Calcium levels. In a smooth muscle the interaction of actin and myosin is controlled by a protein called calmodulin (Tropnin-C molecule is not present is smooth muscle). Calcium-calmodulin complex forms when a single molecule of calmodulin binds to 4 calcium ions.
4) Myosin molecule has a myosin head and a myosin light chain. Myosin light chain has an enzyme called myosin light chain kinase (MLCK). The calcium-calmodulin complex activates the enzyme myosin light chain kinase (MLCK). Calcium-Calmodulin complex is responsible for regulating the cross-bridge cycling in a smooth muscle.
5) MLCK is activated by increased intracellular calciumlevels. Upon activation MLCK phosphorylates the myosin light chain utilizing an ATP molecule. When a phosphate binds to myosin light chain, it activates the myosin head which brings about a conformational change of the myosin head. The myosin head now binds to the exposed myosin binding site on the actin molecule.
6) The myosin binding sites on Actin are covered by troponin and tropomyosin. After binding to its binding site on actin, the myosin head initiates a power stroke which results in movement of the actin filament. In a smooth muscle this cross-bridging of actin and myosin plus subsequent power stroke together result in an increased tension in the smooth muscle. Increased tension of the vascular smooth muscle results in vasoconstriction of the blood vessel.
7) There's another enzyme called myosin light chain phosphatase (MLCP), which has function opposite to that of MLCK. Post the power stroke, MLCP functions to remove the ADP from the myosin molecule. Once the ADP molecule is detached from the myosin head, the myosin head returns to its normal relaxed state. This decreases the tension inside the vascular smooth muscle and there’s vasodilation of the blood vessel.
NOTE: Activation of MLCK results in the contraction of vascular smooth muscle, and the resultant diameter of the vessel is reduced. In contrast, MLCP activation results in relaxation of the vascular smooth muscle and this subsequently results in vasodilation of the blood vessel.
[The steps involved in the vascular smooth muscle contraction aren’t correctly explained in the lecture. The steps explained in the lecture are the ones involved in the skeletal muscle contraction. However, a blood vessel has a smooth muscle component so the steps involved should be those of a smooth muscle excitation-contraction coupling.
In the lecture it’s mentioned that Troponin-C is and tropomyosin molecules are covering the binding site of the myosin heads on the actin molecule. However, Troponin C is absent in smooth muscle. Instead, calmodulin molecule is present in the vascular smooth muscle. With smooth muscle depolarization there’s an influx of calcium ions. The calmodulin molecule (like Troponin molecule in skeletal muscle) binds to four calcium ions. This calcium-calmodulin complex is what’s responsible for activating the MLCK enzyme. The subsequent cross-bridging sequence is similar in both smooth and skeletal muscle.
Also the enzymes MLCK & MLCP are only present in the smooth muscle and not in the skeletal muscle.]
METABOLIC THEORY OF AUTOREGULATION
The metabolic theory proposes that the oxygen delivery to a metabolically active tissue is determined by two factors:
• Presence or absence of oxygen in the tissue.
• Presence or absence of metabolites in the tissue.
Oxygen & Metabolic theory: Putting oxygen into the metabolic theory equation suggests that oxygen delivery can be matched to the oxygen consumption of that tissue by varying the diameter of the arterioles, which in turn alters the blood flow. As a tissue performs active metabolism, it utilizes the oxygen delivered to it via the arterioles. As a result the oxygen levels of the local arteriolar blood tend to drop. This means that less oxygen is available for the arteriolar endothelium and smooth muscle. Within the arteriolar smooth muscle, less oxygen is available for the phosphorylating activity of the MLCK. As a result the actin-myosin cross bridging is disrupted and the arteriolar smooth muscle tends to relax. End result of this cascade is that the arterioles undergo vasodilation and there is a relatively reduced resistance to the flow. Consequently tissue perfusion increases secondary to arteriolar vasodilation and increased flow.
Metabolic Vasodilators & Metabolic theory: Actively metabolizing tissues produce certain vasodilatory metabolites which can regulate the blood flow to the tissue itself. The concentration of these metabolites is directly proportional to the level of metabolic activity performed by that particular tissue. Increased concentration of metabolites results in vasodilatation of the arterioles, which results in decreased resistance to the blood flow. This increased blood flow is in coherence with the increased oxygen demands of the tissue. In contrast, the arterioles constrict if the concentration of these metabolites decrease. Several key vasodilator metabolites are mentioned below:
• Adenosine: ↑Adenosine → + G-stimulatory protein →increased cAMP (cyclic AMP) → - inhibition of MLCK.
As the kinase function of the MLCK is inhibited, the vascular smooth muscle relaxes and vasodilation follows.
• Carbon Dioxide
• H+ ions
• K+ ions
• Lactate
• Prostaglandins: Also uses the G-stimulatory coupled cAMP pathway.
• Prostacyclins
These vasodilator metabolites can be produced both due to oxygen demand or oxygen supply mismatch situations.
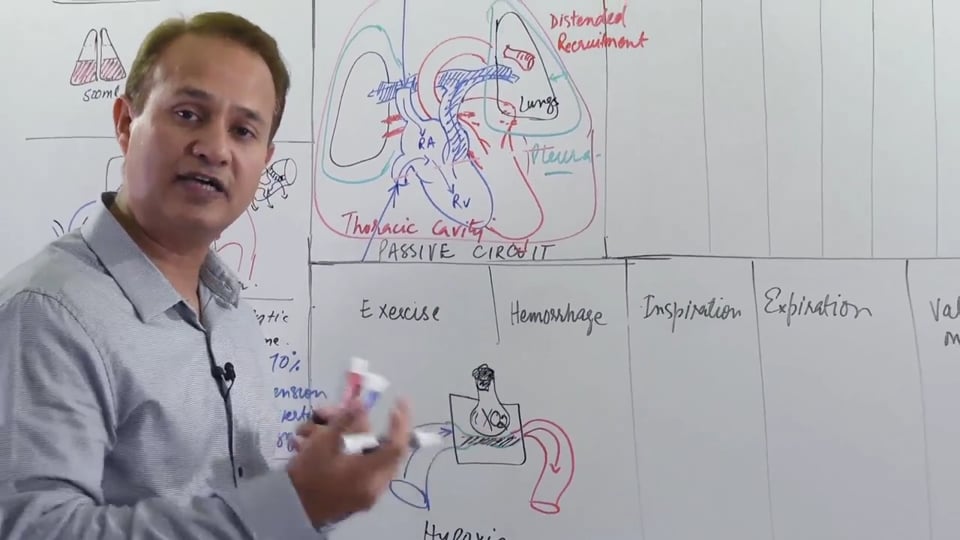
• Oxygen demand mismatch: Active metabolism by the tissue cells utilizes the oxygen available to them. There’s a resultant increase in oxygen demand by the tissues, while the supply remains unchanged. This is what happens in a rapidly exercising muscle cell. In order to match the oxygen demand, the flow to the muscle needs to be increased.
• Oxygen supply mismatch: Alternatively there can be an oxygen supply mismatch. In this case the tissue need remains unchanged but the perfusion to the tissue decreases due to some reason. Following are the situations which can lead to a supply mismatch situation:
▪ High Altitude (decreased atmospheric pressure)
▪ Carbon Monoxide poisoning (CO has greater affinity for Hemoglobin than Oxygen)
▪ Cyanide poisoning (Cyanide inhibits cytochrome c oxidase and renders the electron transport chain non-functional)
▪ Mechanical block to blood vessels perfusing the tissue
▪ Pneumonia (can cause ventilation perfusion mismatch in the lungs, which decreases the flow available to tissues)
In another scenario let’s assume that there is a spontaneous increase the perfusion to a tissue. This increase in perfusion can be secondary to an increase in blood volume (transfusion) or stroke volume (inotropic drugs). In the beginning, there will be an increase in blood flow that will deliver more oxygen for metabolic activity and simultaneously “wash out” the vasodilator metabolites. Consequently, there will be a local dilution of vasodilator metabolites around the tissue. Decreased vasodilator metabolites result in arteriolar vasoconstriction and a compensatory decrease in blood flow back to the normal level.
Role of calcium: when the nerve impulse stimulates NMJ the calcium is released from the sarcoplasmic reticulum causes activation of MLCK and causes vasoconstriction by its action on Gq receptor, alpha 1 receptor and increases the concentration of ITP i.e. inosine triphosphate.
Metabolic theory also explains the phenomena of active hyperaemia and reactive hyperaemia:
• Active Hyperaemia explains that blood flow to a metabolically active tissue is directly proportional to its metabolic needs. For example, as a result of strenuous exercise the metabolic demands of the skeletal muscle are greatly increased. As compensation, the blood flow (perfusion) to the skeletal muscles is readily increased in order to meet the metabolic demands of the tissue. Active hyperaemia can be explained by both the metabolic and the myogenic theories of autoregulation.
• Reactive Hyperaemia refers to an increase in blood flow to a tissue which received a decreased perfusion due to some reason. The reason for decreased perfusion can be arteriolar occlusion of the arterioles supplying the tissue. Over time, due to decreased blood flow the tissue switches to anaerobic means of respiration which creates an oxygen debt situation within the tissue. Also due to occluded blood supply, there’s a build up vasodilator metabolites within the tissue which aren’t washed up due to decreased perfusion. These vasodilator metabolites with time increase in concentration and result in vasodilatation of the arterioles which perfuse the tissue. As the blood supply resolves, the tissue receives a greater than normal perfusion until the oxygen debt situation is resolved. Reactive hyperaemia is governed by the law of compensation of blood flow. Reactive hyperaemia can only be explained by the metabolic theory of autoregulation; the myogenic theory cannot be used to explain it.
MYOGENIC THEORY OF AUTOREGULATION
Myogenic theory of autoregulation suggests that the vascular smooth muscle itself is also responsible for its own control of contraction and relaxation. An inherent property of the smooth muscle is that that it contracts in response to stretch. Thus, if arterial pressure is suddenly increased, the arterioles are stretched and the vascular smooth muscle in their walls contracts in response to this stretch. The decreased arteriolar resistance ensures that the flow doesn't increase significantly. If there's a sudden drop in flow, there's a reduced stress placed on the arterial walls and therefore the vascular smooth muscle relaxes. The compensatory vasodilation ensures that blood flow to the tissue doesn't drop significantly.
There are sodium channels within the vascular smooth muscle cells. These sodium channels are normally closed and are connected to the cytoskeleton of the smooth muscle cell. As the blood flow within the vessel increases, it stretches the blood vessel plus the smooth muscle surrounding the bloodvessel. This stretch will also cause the microtubules within the cytoskeleton to stretch. The stretch on microtubules will create a mechanical pull upon the closed sodium channels and cause them to open. Sodium channels will cause an influx of sodium ions into the smooth muscle cells and bring about depolarization. Result of this cascade is that the vascular smooth muscle contracts and decreases the lumen of the vessel. Decreased lumen will decrease the flow back to the normal.
The concept of reactive hyperaemia is explained above. It's important to remember that reactive hyperaemia cannot be explained in terms of myogenic theory.
THE ROLE OF EDRF, NITRIC OXIDE & ENDOTHELIN IN REGULATING LOCAL BLOOD FLOW
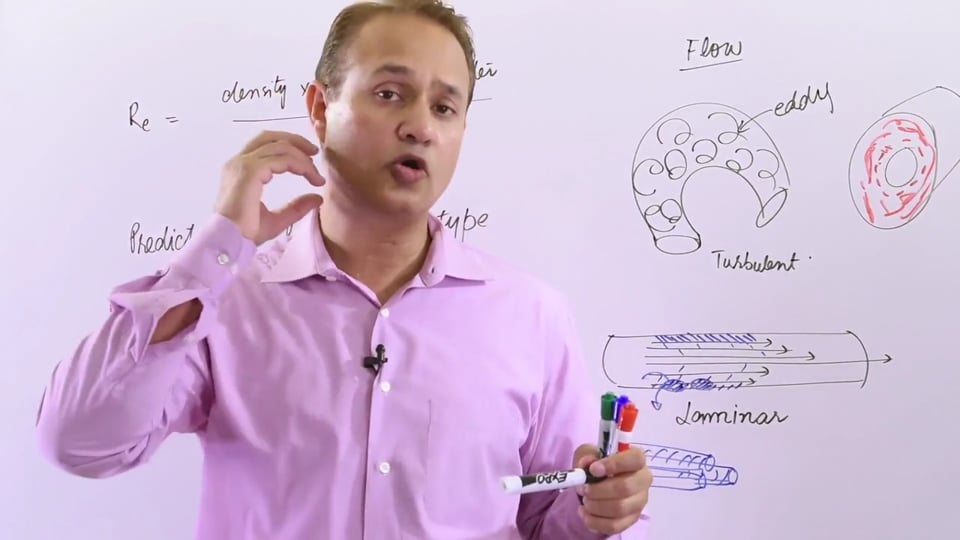
EDRF and Endothelin are chemical substances released by the endothelium which act on the vascular smooth muscle to alter the diameter of vessel. Nitric oxide is one of the most important very important EDRF. Blood travelling at high velocity causes a shearing effect on the wall of the blood vessels as the endothelial cells endure a drag force produced due to friction. This results in a mechanical trigger which stimulates release of nitric oxide.
Nitric oxide, after its release from the endothelium, diffuses into the vascular smooth muscle. Inside the vascular smooth muscle, the NO triggers the guanylate cyclase to convert cGTP to cGMP. The increased levels of cGMP cause activation of the enzyme Myosin Light Chain Phosphatase (MLCP). The activated MLCP enzyme in turn dephosphorylates myosin light chains, which results in relaxation of the contractile apparatus of the blood vessel. As a result, the vessels become dilated.
Angiotensin II receptors are present on both the vessel endothelium and also the smooth muscle surrounding the blood vessel. When Angiotensin II acts directly on the its endothelial receptor, it results in release of NO. This NO causes vasodilation by the mechanism explained above. If the Angiotensin II acts directly on its receptor on the vascular smooth muscle, then it'll cause vasoconstriction of the blood vessel. Angiotensin II receptor on the vascular smooth muscle is Gq coupled, and when bound to this receptor, Angiotensin II can act as a powerful vasoconstrictor.
Sildenafil is a drug that is used to treat erectile dysfunction. It is a Phosphodiesterase (PDE-5) inhibitor. Normally, PDE-5 is an enzyme that binds to and cleaves cGMP. As a result, the half-life of cGMP is reduced as its levels fall. Sildenafil acts by binding to PDE-5 and antagonizes its function (decreasing cGMP levels). With PDE-5 inhibited, the cGMP levels remain high for a longer period of time. The effect of parasympathetic NS and acetylcholine results in release of NO. This Nitric Oxide diffuses inside the vascular smooth muscle of the arteries which are responsible for penile erectile tissue perfusion. Within the vascular smooth muscle, the NO results in formation of large quantities of cGMP. Inhibited PDE-5 can no longer cleave the cGMP which stays for a longer time. cGMP activates enzyme MLCP which promotes relaxation of the vascular smooth muscle. Therefore, the penile vasculature remains dilated and engorged with blood and the erection is maintained for a longer period.
Endothelin is released from damaged endothelium. After its release, Endothelin binds to its receptor on the vascular smooth muscle. Endothelin receptor is a Gq coupled receptor, which upon activation inhibits the MLCP enzyme. The inhibition of MLCP enzyme promotes contraction of the vascular smooth muscle and the vessel undergoes vasoconstriction. Hence the vascular diameter is decrease to reduce the blood flow through the damaged vessel. This is important in order to prevent blood loss at the site of damaged endothelium.
Another important function of EDRF is that these not only increase the local blood flow. EDRF also causes vasodilation of upstream blood vessels for the tissues that need greater perfusion. This makes sure that overall blood flow is directed to those tissues which are in need of greater perfusion due to their metabolic demands.
In this video we will learn about :
1. Blood flow and its calculation.
2. Long term regulation of blood flow.
3. Intrinsic acute regulation of blood flow.
4. Myogenic theory of blood flow control
5. Metabolic theory of blood flow control.
6. Vascular control of blood flow.
No credit card information needed.












Write A New Comment
2 Comments
cabrera.irwin@*.com
Sep 18 2021, 2:12 am
Hello Doctor, I'd like to point out what I believe to be a small error in this video that might confuse the audience. In minute 34:19 you say that NO leads to activation of cGMP, which goes on to block MLCP causing contraction of smooth muscle cells. Even though blocking MLCP would indeed lead to vasoconstriction, I think the role of NO in response to shear stress would be to vasodilate, mediated by NO activating cGMP, which in turn activates PKG. PKG would then go and prevent Calcium influx from voltage-dependent calcium channels, prevent IP3 meadiated release of calcium, activate SERCA to sequester calcium into the sarcoplasmic reticulum, and finally, indirectly inhibit MLCK. These 4 events would ultimately lead to smooth muscle relaxation and thus vasodilation.
Please correct me if I'm wrong. Thank you Doctor.
siddiq_official1308@*.com
Apr 22 2020, 7:13 am
Sir , you talked anout the NMJ in this lecuture . but the vascular smooth muscles dont have innervaton right , could you please entighten about this concept ?